
On Thursday, 25 March, GLG, in partnership with the American Club, held an informal breakfast discussion with Professor Ivan Hung, co-convenor of the Expert Committee on Clinical Events Assessment Following Covid-19 Immunisation. During the breakfast, Professor Hung shared his candid perspective on the variety of vaccines supplied to Hong Kong.
Topics included:
- Overview of the vaccines supplied to Hong Kong
- Results of clinical trials and recommendations
- Distribution timeline, priorities, and logistical challenges
This article summarizes Dr. Hung’s presentation click on this link to read the Q&A session that followed.
Hong Kong has done well with COVID-19 compared with the rest of the world due to its painful experience with SARS in 2003. The city’s mortality rate is around only 1.8%, with peak ICU occupancy of only 50%. Comparatively, New York had more than 100% occupancy. In Hong Kong now it’s probably down to about 2%.
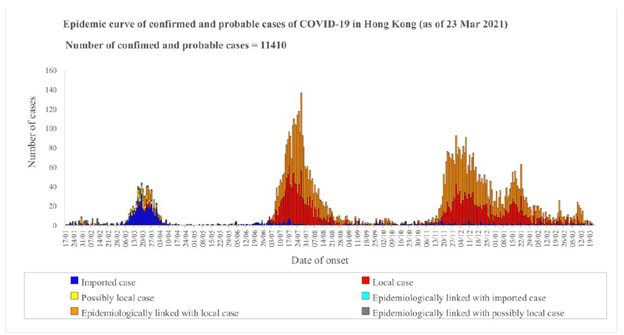
At the beginning of the pandemic, most of Hong Kong’s cases were imported from China just before Chinese New Year in 2020. It was quiet for a long time until the second wave, which originated in students coming back from the United Kingdom and United States. The third wave was probably due to sailors and pilots who had been exempted from testing. The fourth wave was the so-called dancing cohort, which, unfortunately, had been quietly spreading for a long period, so when infection control measures were relaxed, there was a burst of cases. It took four months to contain the fourth wave.
Still, Hong Kong has been doing a relatively good job right from the beginning containing the virus. We have been intensely surveilling returnees, and quarantining and hospitalizing patients even with milder symptoms. Infection control measures are extremely important — we have universal masking, social distancing, and easy and accessible diagnostics using saliva tests. Deferral saliva allows minimal input from healthcare workers, relying on just the subjects to provide a sample. A study from our group and Yale proved that during the first 10 days, a good saliva sample is better to detect the virus than the nasopharyngeal swab. Beyond 10 days when the viral load starts dropping, mucopolysaccharidoses perform better than saliva.
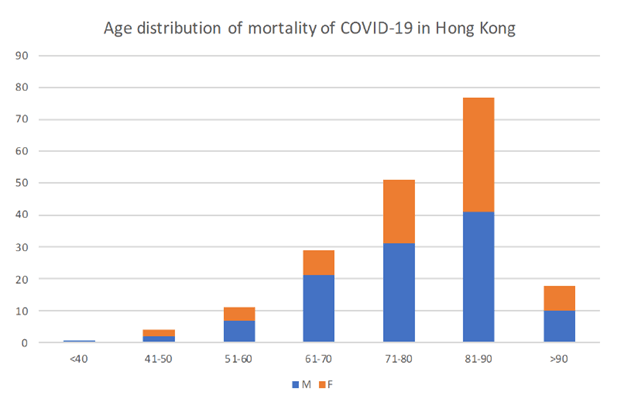
Perhaps surprisingly, most of Hong Kong’s cases are younger patients. But in terms of hospitalizations and high mortality, the age group between 70 and 90 is most at risk, with slightly more males. People with diabetes, cardiovascular or renal issues, or post-transplant patient malignancy are also at high risk of developing complications. Diabetic patients take a relatively long time shedding the virus, up to beyond six weeks, and are not able to develop antibodies, so the risk of death is higher. This, of course, is very important because of the pathogenesis of COVID-19. We know that from the first week or so, the patient has a rise in the virus and then sheds it. For severe cases, they have a relatively prolonged hyper-inflammatory phase in the second week.
If these cohort patients are able to be hospitalized and treated, we get the virus down and are able to stop these subsequent hyper-inflammatory phases. The aim is to give early treatment, hopefully within 48 hours from the onset of symptoms, so that we can control the cytopathic damage and bacterial infection by suppressing the virus. This reduces the viral shedding and transmission as well.
In Hong Kong, we hospitalize everyone, treating people with three drugs: the interferon beta-1b, lopinavir-ritonavir (Kaletra), and ribavirin. By starting this treatment early on, we’re able to suppress the viral load within a very short period. Clinically, patients respond much better as well. For patients in their second week of infection, plasma harvested from recovered patients containing high levels of antibodies is used to suppress the viral load. Monoclonal antibodies are also created from a recovered patient and are used as a one-shot dose to treat patients who have developed a so-called moderate to severe disease.
The Importance of Vaccines
Unfortunately, SARS-CoV-2 is a smart virus. Along with variants in the United Kingdom and South Africa, it’s just been reported there are two new ones in India. Nevertheless, with vaccines, even though they may not provide 100% protection against the variants, people will have above 60% to 70% protection. The virus will probably stay with us for a long time, but with herd immunity building up, even if someone is infected, it will be very mild.
Hong Kong is different from the rest of the world. We have had relatively few cases in the whole population. That causes a problem because it means many people must get vaccinated. The city probably needs to get up to 70% of the population through either vaccination or natural infection to achieve herd immunity. Hopefully, we’ll be able to achieve that before the end of the year. Once a populace gets to above 50%, cases drop dramatically, like in the United Kingdom.
Dozens of clinical trials for vaccines are ongoing at various stages. Some of them already have approval for emergency use by various authorities. Basically, there are four platforms for vaccines:
- The relatively new mRNA vaccines, such as from Pfizer-BioNTech and Moderna, stimulate both the T-cells and B-cells, providing the neutralizing antibody with good cell-mediated immunity stimulation. They have high efficacy, of about 90% to 95%, and allow for cross-protection against variants. Side effects include fatigue, myalgia, or fever, and people with allergies are urged to get screened for reactions to polyethylene glycol before getting vaccinated. Those who have been vaccinated show far fewer cases and need to be hospitalized much less.
- The adenovirus vector vaccines from AstraZeneca and Johnson & Johnson use a relatively new platform. They use chimpanzee adenovirus as the vector to carry the spike protein. They have good efficacy of above 90%, but with slightly higher side effects including fatigue and headache.
- The third is the new platform from Novavax of using a nanoparticle protein to carry the spike protein, which is still undergoing trials. Phase three trials in South Africa and the United Kingdom show that there’s 60% protection against the SA variants and 86% protection against the UK variants, with very good neutralizing antibody and cell-mediated immunity.
- Finally, the conventional inactivated vaccine made by Sinovac and India’s Bharat Biotech are conventional and safe. They’re made from inactivating the whole virus, and they neutralize the antibody response with few side effects. Unfortunately, the cell-mediated immunity is relatively weak. Phase three studies in Brazil show 62% efficacy and currently no data against variants.
One more potential vaccine to mention is the world’s first intranasal vaccine being developed by HKU that is in phase one trials. We have already enrolled a patient who is going to receive the first dose in early April. It uses inactivated influenza H1 as a carrier for the spike protein of COVID-19. It works a bit like the flu mist taken for influenza. This is extremely good because people don’t need to be given an intramuscular vaccination via injection. This technology has been shown in the animal study to assimilate the IGA mucosal antibody that prevents the virus from getting in through the nasal passage.
Hong Kong has been growing its vaccination program. There was the hiccup with BioNTech’s loose vaccine caps, but that doesn’t affect the safety and the efficacy of vaccines. It will likely delay people’s second doses, but that lowers the chances of side effects and the efficacy will probably be even better.
The best vaccine is the one that can give people lifelong protection with just one single dose. But with this novel virus, you can’t do that. We need two doses, and maybe a third or the fourth dose annually until we build up a reasonably good herd immunity. Of course, a good vaccine can not only prevent symptomatic or severe disease but also prevent transmission by stopping carriage of the virus in your nose. That’s why it’s extremely important for people to get vaccinated. Hopefully, by achieving herd immunity, we will be able to basically resume normal life.
About Professor Ivan Fan Ngai Hung
Professor Ivan Fan Ngai Hung is currently Ru Chien and Helen Lieh Endowed Professor in Health Sciences Pedagogy, Professor of Medicine and Assistant Dean (Admissions), Chief of the Division of Infectious Diseases, Department of Medicine, LKS Faculty of Medicine, The University of Hong Kong, and Honorary Consultant in Queen Mary Hospital, Hong Kong. He is also Clinical Professor and Chief-of-Service of the Department of Infectious Diseases and Clinical Microbiology at the HKU-Shenzhen Hospital.
订阅 GLG 洞见趋势月度专栏
输入您的电子邮件,接收我们的月度通讯,获取来自全球约 100 万名 GLG 专家团成员的专业洞见。